
Wegovy HD (Semaglutide 7.2 mg): The Workhorse Just Found Another Gear

I’ve been following the incretin space closely — you know this if you read my retatrutide and amycretin deep dives.
Those two stories were about new molecules. Triple agonism. Dual GLP-1/amylin agonism. Brand new mechanisms chasing brand new numbers. And they’re genuinely exciting.
But the story I want to tell today is different. It’s not about a new molecule at all.
It’s about taking a molecule we already know extremely well — semaglutide, the drug behind Ozempic and Wegovy — and simply turning the dose up. And the result is the highest weight loss ever delivered by a Wegovy injection.
That’s Wegovy HD. And unlike almost everything else I write about, this one isn’t investigational. It’s approved. It’s launching. It’s real.
Let me break down everything we know.
What Is Wegovy HD?
Wegovy HD is once-weekly injectable semaglutide at a 7.2 mg dose — more than double the 2.4 mg dose most people know as “Wegovy.”
Drug class: GLP-1 receptor agonist
Route: Once-weekly subcutaneous injection (single-dose pen)
Developer: Novo Nordisk
Phase: Approved (STEP UP phase 3b programme)
Status: FDA approved (19 March 2026). Already approved for adults with obesity in the EU and UK. This is the real deal — not something your online dealer smuggled in from a peptide website 😜
Here’s how it fits alongside the drugs I’ve already covered:
- Semaglutide (Ozempic/Wegovy/Rybelsus): activates 1 receptor — GLP-1
- Tirzepatide (Mounjaro/Zepbound): activates 2 receptors — GLP-1 + GIP
- Retatrutide (investigational): activates 3 receptors — GLP-1 + GIP + Glucagon
- Amycretin (investigational): activates 2 receptors — GLP-1 + Amylin
- Wegovy HD: the same single GLP-1 receptor as always — just at a higher dose
That last point is the whole story. No new receptor. No new pathway. Same molecule, same mechanism — just more of it. And the question the STEP UP programme set out to answer was beautifully simple: if semaglutide works, does more semaglutide work better?
The answer, it turns out, is yes.
Mechanism of Action: Nothing New, and That’s the Point
I won’t spend long here, because if you’ve read my previous pieces you already know the GLP-1 story cold.
Semaglutide is a GLP-1 receptor agonist coupled to a fatty diacid chain that extends its half-life to roughly a week, which is what makes once-weekly dosing possible. It reduces appetite centrally through the hypothalamus and brainstem, slows gastric emptying, and enhances glucose-dependent insulin secretion. It’s the backbone of modern incretin therapy and the foundation everything else is built on.
Wegovy HD doesn’t change any of that. It’s the exact same molecule as Wegovy 2.4 mg. What changes is the dose — 7.2 mg once weekly instead of 2.4 mg.
Why does that matter? Because for years the field assumed 2.4 mg was roughly the ceiling for semaglutide in obesity. STEP UP was designed to test whether pushing past that ceiling would deliver more weight loss, or just more side effects with no additional benefit.
The elegance here is that there’s no new pharmacology to explain. This is a dose-optimisation story — and dose-optimisation stories don’t get enough love in a space obsessed with novel mechanisms.
The Clinical Data: The STEP UP Programme
Everything you need to know about Wegovy HD comes from two phase 3b trials: STEP UP (obesity without diabetes) and STEP UP T2D (obesity with type 2 diabetes). Both ran for 72 weeks. Both were published in The Lancet Diabetes & Endocrinology and presented at ADA.
STEP UP — Obesity Without Diabetes
Study: Once-weekly semaglutide 7·2 mg in adults with obesity (STEP UP): a randomised, controlled, phase 3b trial. The Lancet Diabetes & Endocrinology. 2025.
Design: Randomised, double-blind, placebo-controlled, superiority phase 3b trial. 1,407 adults aged 18 and older with a BMI ≥30 and no diabetes. Participants were randomised to once-weekly subcutaneous semaglutide 7.2 mg, semaglutide 2.4 mg, or placebo, all alongside lifestyle intervention, for 72 weeks.
I want to flag the design here, because it’s smart. This isn’t semaglutide 7.2 mg versus placebo — that would have been the easy win. It’s a three-arm trial with semaglutide 2.4 mg as an active comparator. In other words, Novo put the new high dose head-to-head against its own established dose. That’s how you actually prove the extra dose is doing something.
Efficacy Results (at 72 weeks):
Using the efficacy estimand (the treatment effect if everyone adhered to treatment):
- Placebo: −2.4%
- Semaglutide 2.4 mg: −17.5%
- Semaglutide 7.2 mg: −20.7%
Using the treatment-regimen estimand (the effect regardless of adherence), semaglutide 7.2 mg delivered −18.7%.
So the headline is a mean weight loss of roughly 21% — the highest ever reported for a Wegovy injection, and a clear step up from the 17.5% delivered by the 2.4 mg dose in the same trial.
Categorical weight loss is where it gets striking. On semaglutide 7.2 mg:
- Over 90% of participants achieved ≥5% weight loss
- Approximately one in three (33.2% on the efficacy estimand) achieved ≥25% weight loss
For comparison, only 16.7% of the 2.4 mg group and 0.0% of the placebo group hit that ≥25% threshold. Let me put that in context — a quarter of your body weight lost, from a GLP-1 injection, in about a third of patients. Numbers we used to associate with bariatric surgery, now showing up in a subset of patients on a drug we’ve been prescribing for years.
Safety: The most common adverse events were gastrointestinal — nausea, vomiting, diarrhoea, constipation, abdominal pain — mostly mild to moderate and consistent with everything we already know about the semaglutide class. No new or unexpected safety signals emerged.
The one signal worth watching: altered skin sensation, described as dysaesthesia (tingling, numbness, sensitivity, or burning). It occurred more frequently at the 7.2 mg dose than at lower doses, but was generally mild and typically resolved on its own or with a dose reduction. If that sounds familiar, it should — a similar dysaesthesia signal showed up with retatrutide at its top dose. It seems to be a feature of pushing these drugs harder.
STEP UP T2D — Obesity With Type 2 Diabetes
Study: Lingvay I, Garvey WT, Wharton S, et al. Once-weekly semaglutide 7·2 mg in adults with obesity and type 2 diabetes (STEP UP T2D): a randomised, controlled, phase 3b trial. The Lancet Diabetes & Endocrinology. 2025;13(11):935–948.
Design: Randomised, double-blind, controlled, three-arm, parallel-group phase 3b trial across 68 sites in eight countries — including Bulgaria 🇧🇬, which always makes me happy to see. 512 adults with a BMI ≥30 and type 2 diabetes (HbA1c 7.0–10.0%) were randomised 3:1:1 to semaglutide 7.2 mg (n=307), semaglutide 2.4 mg (n=103), or placebo (n=102) for 72 weeks.
Efficacy Results (at 72 weeks):
- Mean weight loss (efficacy estimand): 14.1% on semaglutide 7.2 mg; 13.2% on the treatment-regimen estimand
- 21.3% of patients achieved ≥20% weight loss
- Superior to placebo in body weight, waist circumference, and HbA1c
As always in the diabetes population, the weight loss numbers come in lower than in the non-diabetes trial — 14.1% versus 20.7%. This is a consistent pattern across the entire incretin class: people with type 2 diabetes lose less weight on these drugs than people without it. It’s one of the enduring puzzles of the field. An exploratory analysis suggested the 7.2 mg dose may offer additional weight benefit over 2.4 mg in this population too, though it was framed cautiously.
Safety: Gastrointestinal events were the most common and were dose-related — 70.8% on semaglutide 7.2 mg, 61.2% on 2.4 mg, and 42.8% on placebo. Dysaesthesia was again more common on the 7.2 mg dose. Importantly, no severe hypoglycaemic episodes were reported with either semaglutide dose — which matters a lot in a diabetes population.
The Regulatory Story: A 54-Day Approval!
This part genuinely surprised me, and it deserves attention beyond the efficacy numbers.
Wegovy HD was approved by the FDA on 19 March 2026 — just 54 days after filing. That is extraordinarily fast by any historical standard.
It happened under the FDA’s Commissioner’s National Priority Voucher (CNPV) pilot programme, which accelerates review for products addressing critical US national health priorities. Wegovy HD was the fourth product approved under the programme and the first GLP-1 therapy to go through it.
Novo launched Wegovy HD in a single-dose pen in the US in April 2026. It doesn’t replace Wegovy 2.4 mg — it complements it, giving prescribers a higher-efficacy option for patients who need or want more. Semaglutide 7.2 mg is already approved for adults with obesity in the EU and the UK, with regulatory decisions on the single-dose pen format expected in the second half of 2026.
I have thoughts about a 54-day approval, and I’ll come back to them.
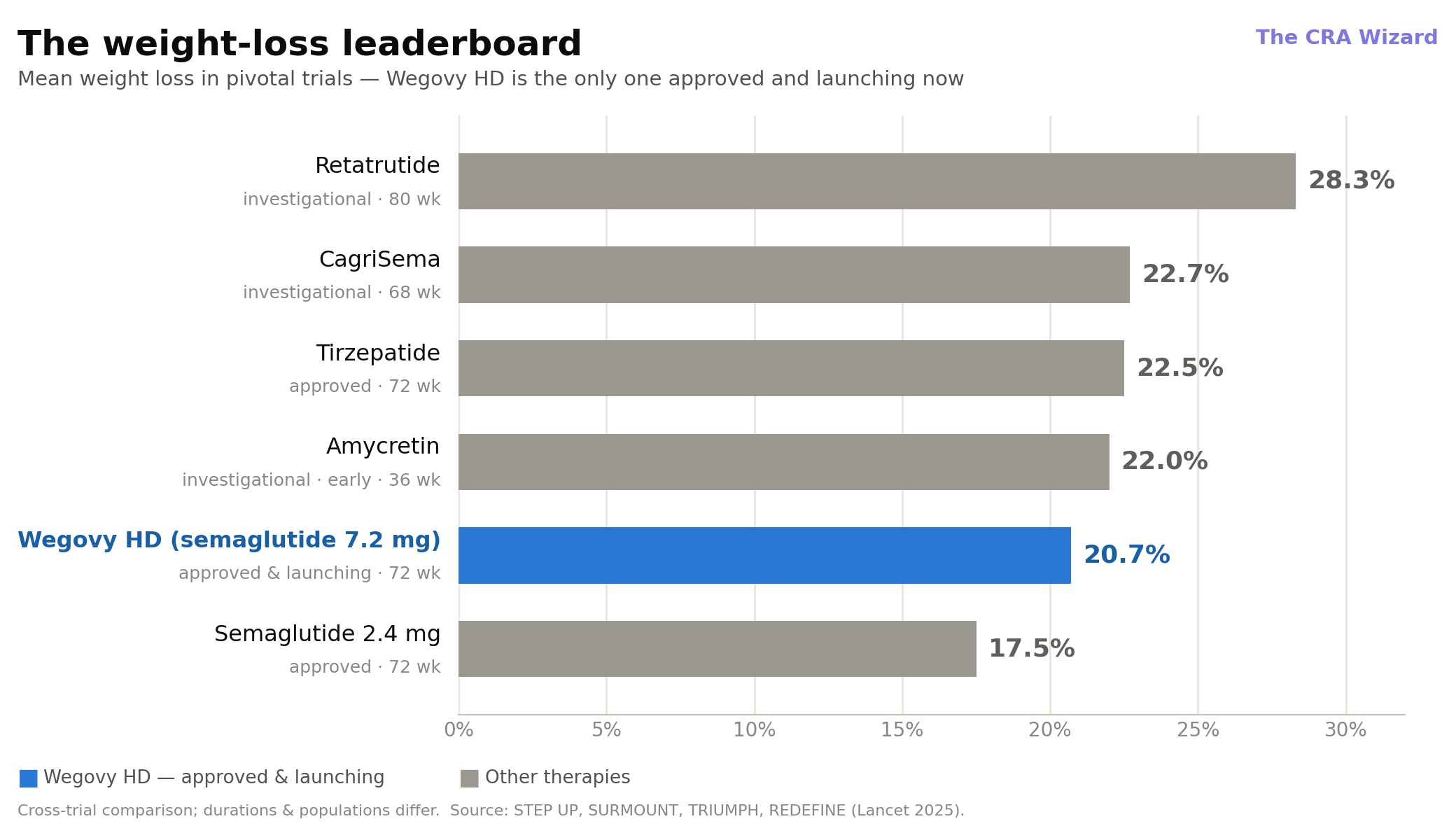
The Competitive Landscape: Where Does 21% Actually Sit?
Let me put Wegovy HD in context against the molecules I’ve been covering, because the number that matters is that ~21%.
Retatrutide (Eli Lilly): Triple agonist. 28.3% weight loss at 80 weeks in phase 3 (TRIUMPH-1), up to 30%+ with longer treatment. The clear efficacy leader. Injection-only, still investigational.
Tirzepatide (Eli Lilly): Dual GLP-1/GIP agonist. Around 22.5% at 72 weeks. Approved as Zepbound. The current standard-bearer for approved therapy.
Amycretin (Novo Nordisk): GLP-1/amylin dual agonist. Up to 22% at 36 weeks in early trials, with an oral formulation in development. Investigational, phase 3 just starting.
CagriSema (Novo Nordisk): Cagrilintide + semaglutide. 22.7% at 68 weeks, but missed non-inferiority against tirzepatide in REDEFINE 4.
Wegovy HD (Novo Nordisk): GLP-1 only, high dose. ~21% at 72 weeks. Approved and launching now.
Here’s the honest read. On raw efficacy, Wegovy HD does not top the leaderboard. Retatrutide’s 28% is in a different league, and tirzepatide, amycretin, and CagriSema all edge it out on the headline number.
But — and this is the part I think people miss — Wegovy HD is approved and available today, at least in the US, using a molecule with the deepest real-world safety and outcomes track record in the entire class. Retatrutide and amycretin are years from your pharmacy. Wegovy HD is months.
And remember what semaglutide 2.4 mg already carries in its label: cardiovascular risk reduction, and a MASH indication. That’s an enormous evidence base that a brand-new molecule simply doesn’t have yet. Wegovy HD inherits all of that credibility and adds another gear of weight loss on top.
Sometimes the winning move isn’t a new molecule. It’s getting more out of the one you’ve already proven.
What Excites Me — And What I’m Watching
Here’s my honest take.
What excites me is the strategic elegance of this. While everyone in the space — myself included — has been mesmerised by triple agonists and dual agonists and oral peptides, Novo quietly asked whether the drug we already trust had more to give. The answer was 3 more percentage points of mean weight loss and a doubling of the proportion of patients hitting ≥25%. That’s not nothing. That’s a lot, actually, from a molecule we thought we’d maxed out.
I also love that STEP UP used semaglutide 2.4 mg as an active comparator instead of taking the easy placebo-only win. That’s how you prove a higher dose earns its place.
What I’m watching:
1. The dysaesthesia signal. More weight loss at a higher dose is expected. So is more GI burden and this altered-skin-sensation signal. The risk-benefit conversation at 7.2 mg will be more nuanced than at 2.4 mg, and prescribers will need to have it honestly.
2. That 54-day approval. I’m a clinical research person, so a two-month regulatory review makes me sit up. On one hand, this is the same molecule with years of data behind it — the risk profile is exceptionally well characterised, and fast-tracking a known quantity makes sense. On the other hand, I always want to see the full published safety dataset, real-world evidence at the higher dose, and long-term follow-up. Speed is wonderful when the evidence base underneath it is deep. Here, I think it mostly is — but I’ll keep watching.
3. Access and cost. A higher-efficacy semaglutide is only meaningful if patients can actually get it and afford it. For those of us in Eastern Europe, the single-dose-pen decisions in the EU and UK later in 2026 are the milestone that actually matters for real-world availability here.
4. The diabetes gap. 20.7% without diabetes, 14.1% with it. That persistent gap across the whole class is one of the most interesting open questions in metabolic medicine, and I’d love to understand the mechanism better.
The Bigger Picture
I keep coming back to the same thought.
We’re living through a moment where the obesity conversation is dominated by what’s next — the triple agonist, the oral pill, the novel receptor. And that excitement is justified. Retatrutide and amycretin are genuinely going to change things.
But Wegovy HD is a useful reminder that progress in metabolic medicine isn’t only about inventing new molecules. Sometimes it’s about deeply understanding the ones we already have, and having the discipline to run the trial that proves you can push them further.
Retatrutide showed us the ceiling might be near 30%. Amycretin is asking whether we can make effective therapy as simple as a daily pill. And Wegovy HD is quietly saying: don’t forget the workhorse still has another gear — and it’s the one you can actually prescribe today.
The clinical researcher in me loves the clean three-arm design that proved the point.
The pharmacist in me appreciates a higher-efficacy option built on the safest, best-characterised molecule in the class.
And the evidence nerd in me is going to keep one eye on that dysaesthesia signal and that remarkably fast approval.
This is metabolic medicine’s moment. And it’s just getting started. ✌️
Key References
1. Once-weekly semaglutide 7·2 mg in adults with obesity (STEP UP): a randomised, controlled, phase 3b trial. The Lancet Diabetes & Endocrinology. 2025. [PubMed](https://pubmed.ncbi.nlm.nih.gov/40961952/) · [Lancet](https://www.thelancet.com/journals/landia/article/PIIS2213-8587(25)00226-8/abstract)
2. Lingvay I, Garvey WT, Wharton S, et al. Once-weekly semaglutide 7·2 mg in adults with obesity and type 2 diabetes (STEP UP T2D): a randomised, controlled, phase 3b trial. The Lancet Diabetes & Endocrinology. 2025;13(11):935–948. [Lancet](https://www.thelancet.com/article/S2213-8587(25)00225-6/abstract)
3. Novo Nordisk Press Release: Wegovy® HD (semaglutide 7.2 mg) approved in the US, providing 20.7% mean weight loss. 19 March 2026. [GlobeNewswire](https://www.globenewswire.com/news-release/2026/03/19/3259259/0/en/Novo-Nordisk-A-S-Wegovy-HD-semaglutide-7-2-mg-approved-in-the-US-providing-20-7-mean-weight-loss.html)
4. FDA Press Announcement: FDA Approves Fourth Product Under National Priority Voucher Program, Higher Dose Semaglutide. March 2026. [FDA](https://www.fda.gov/news-events/press-announcements/fda-approves-fourth-product-under-national-priority-voucher-program-higher-dose-semaglutide)
5. STEP UP clinical trial record. ClinicalTrials.gov, NCT05646706. [ClinicalTrials.gov](https://clinicaltrials.gov/study/NCT05646706)
---
Disclaimer: Wegovy® HD (semaglutide 7.2 mg) is approved by the US FDA and in the EU and UK for chronic weight management in adults with obesity. The data presented here comes from published clinical trials and company press releases. This article is for educational and informational purposes only and does not constitute medical advice. Always consult a qualified healthcare professional before starting, stopping, or changing any medication.