
Amycretin: The Oral Obesity Pill That Could Change Everything About Access to Metabolic Medicine

What if effective obesity treatment didn’t require an injection?
That’s the question Novo Nordisk is betting its future on. And the molecule at the center of that bet is amycretin.
I’ve been following the incretin space closely — you know this if you read my retatrutide deep dive. But amycretin is a different kind of story. It’s not about chasing the highest possible weight-loss number. It’s about something arguably more important: making effective metabolic therapy accessible to the millions of patients who will never self-inject.
Let me break down everything we know so far.
What Is Amycretin?
Amycretin (also known as zenagamtide, development code NN9487) is a novel, first-in-class, unimolecular dual agonist that simultaneously activates two receptor systems: GLP-1 receptors and amylin receptors.
Drug class: GLP-1/Amylin receptor dual agonist
Route: Once-weekly subcutaneous injection AND once-daily oral tablet
Developer: Novo Nordisk
Phase: Phase 3 (AMAZE program — obesity; Phase 2b completed in T2D)
Status: Investigational — not approved by FDA or EMA
Here’s what makes it different from everything else on the market and in the pipeline:
- Semaglutide (Ozempic/Wegovy/Rybelsus): GLP-1 only
- Tirzepatide (Mounjaro/Zepbound): GLP-1 + GIP
- Retatrutide (investigational): GLP-1 + GIP + Glucagon
- Amycretin: GLP-1 + Amylin
Different receptor pairing. Different mechanism. And critically — available as a pill.
The Amylin Story: Why This Receptor Matters
Most people in the metabolic medicine space are familiar with GLP-1. But amylin is the less-discussed hormone that could be just as important.
Amylin is a peptide hormone co-secreted with insulin from pancreatic beta cells after eating. It does three things that matter for obesity:
1. It signals satiety through the brainstem. Amylin acts primarily on the area postrema (AP) and nucleus of the solitary tract (NTS) — brain regions that sit outside the blood-brain barrier and directly sense circulating hormones. When amylin activates these areas, it triggers a feeling of fullness during and after a meal. This is different from GLP-1’s mechanism, which primarily reduces the drive to eat and the reward value of food through hypothalamic and mesolimbic circuits.
2. It slows gastric emptying. Similar to GLP-1, but through a distinct neural pathway.
3. It suppresses post-meal glucagon secretion. This helps prevent the blood sugar spikes that drive insulin resistance over time.
Here’s the key insight: amylin and GLP-1 suppress appetite through complementary but non-overlapping pathways. GLP-1 reduces hunger and food reward. Amylin accelerates the onset of fullness. Combine them in one molecule and you get broader, more robust appetite suppression than either alone.
That’s the pharmacological rationale behind amycretin.
Wait — Isn’t There Already a Wegovy Pill? How Is Amycretin Different?
This is probably the most important question to address upfront, because I see a lot of confusion about this online.
Yes, there is now an oral Wegovy. The FDA approved the Wegovy pill (oral semaglutide 25 mg, once daily) in late 2025, and it launched in the US in early January 2026. It’s the first oral GLP-1 therapy approved for weight management. In the OASIS 4 Phase 3 trial, it delivered 16.6% mean weight loss at 64 weeks. That’s a meaningful result and a genuine milestone — the first time patients could access an effective obesity medication without an injection.
So if we already have an oral obesity pill, why does amycretin matter?
Because they are fundamentally different drugs.
Oral Wegovy = oral semaglutide = a pure GLP-1 receptor agonist. One receptor. Same molecule as injectable Wegovy, just delivered as a pill.
Amycretin = a unimolecular dual agonist targeting GLP-1 AND amylin receptors. Two receptors. Two distinct appetite-suppression pathways. A completely different molecule.
Both are made by Novo Nordisk. Both oral formulations use SNAC (sodium N-[8-(2-hydroxybenzoyl)amino]caprylate) — an absorption enhancer that allows peptide drugs to survive the stomach and get absorbed through the gastric lining. (Note: the subcutaneous formulation of amycretin does not use SNAC — it’s injected directly and doesn’t need an absorption enhancer.)
So the oral delivery platform is similar. The molecule and mechanism are fundamentally different.
Think of it this way: oral Wegovy is Novo’s current-generation oral obesity medication. Amycretin is their next-generation one — designed to potentially deliver more weight loss by targeting an additional receptor system that semaglutide doesn’t touch.
And the early data suggests that difference matters. At Novo Nordisk’s 2024 Capital Markets Day, they reported that oral amycretin achieved a 13% weight reduction at 12 weeks — compared to 6% with oral semaglutide at the same time point. That’s more than double the pace.
Of course, we’re comparing a Phase 1 result with 12 weeks of data against an approved drug with full Phase 3 evidence. The oral Wegovy 16.6% at 64 weeks is the benchmark amycretin will need to beat over a full treatment course. But the early trajectory is compelling.

How Is Amycretin Different from Rybelsus?
While we’re at it — Rybelsus is also oral semaglutide, but at lower doses (7 mg and 14 mg) and approved only for type 2 diabetes, not for weight management. Oral Wegovy uses a higher 25 mg dose specifically optimized for obesity. Same molecule, different dose and indication.
Amycretin is a completely different molecule from both. The dual GLP-1/amylin mechanism adds a distinct appetite-suppression pathway that neither Rybelsus nor oral Wegovy can access.
Mechanism of Action: The Science Behind the Dual Agonism
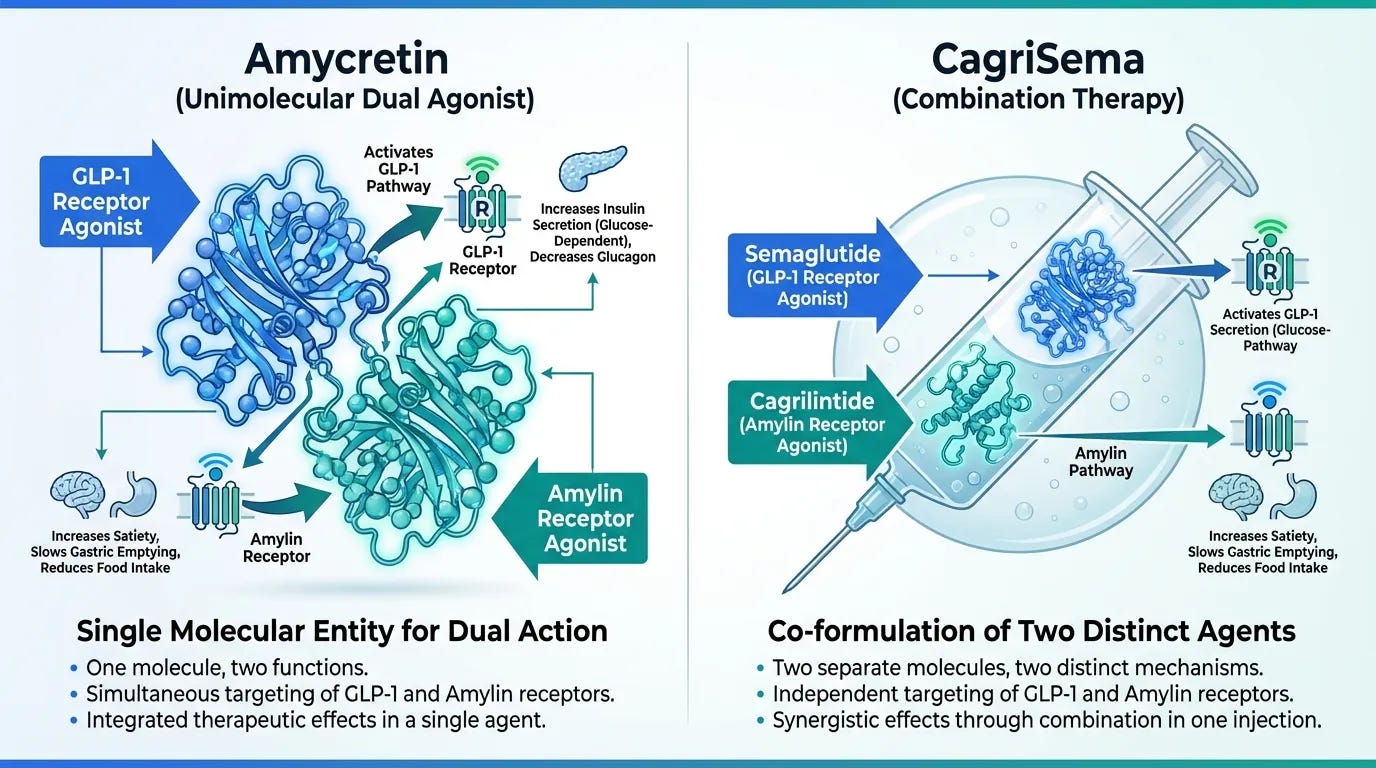
Amycretin is a single peptide engineered from two covalently linked analogs — one derived from GLP-1, one from amylin. It’s not a combination of two drugs (like CagriSema, which is cagrilintide + semaglutide mixed together). It’s one molecule that talks to two receptors.
GLP-1 Receptor Pathway
- Reduces hunger drive centrally (hypothalamus, brainstem)
- Decreases the reward value of food (mesolimbic system)
- Enhances glucose-dependent insulin secretion
- Slows gastric emptying
Amylin Receptor Pathway
- Induces satiety through the area postrema and NTS
- Activates POMC neurons (pro-satiety) and suppresses NPY/AgRP neurons (pro-hunger) in the arcuate nucleus
- Additional gastric emptying delay through distinct neural circuits
- Suppresses post-prandial glucagon secretion
- May contribute to leptin resensitization
The combination of these two pathways produces what researchers describe as broader modulation of neuroendocrine appetite control — meaning amycretin hits more of the biological “switches” that drive eating behavior than a GLP-1-only drug can reach.
The Clinical Data: Everything Published So Far
Phase 1 — First-in-Human (Oral Formulation)
Published: The Lancet, June 2025
Participants: 144 adults with overweight or obesity (BMI 25.0–39.9), no diabetes
Duration: Up to 12 weeks
Dosing: Once-daily oral amycretin, up to 2 × 50 mg
Results:
- 50 mg dose: −10.4% mean body weight change
- 2 × 50 mg dose: −13.1% mean body weight change
- Placebo: −1.2%
13% weight loss in 12 weeks. From a pill. With no plateau in sight — the weight-loss curves were still trending downward when the study ended.
Safety: 62% of participants reported treatment-emergent adverse events. GI events were most common (nausea, vomiting, decreased appetite). All mild to moderate. No deaths. No serious unexpected signals.
Phase 1b/2a — Subcutaneous Formulation (Obesity)
Published: The Lancet, June 2025
Participants: 125 adults with overweight or obesity (BMI 27.0–39.9), aged 18–55
Duration: Up to 36 weeks
Dosing: Once-weekly subcutaneous amycretin, up to 60 mg
Results:
- Up to 22% absolute weight loss at 36 weeks (highest dose group)
- Placebo-adjusted difference: approximately 24%
- No weight-loss plateau observed at study end
Safety: 81% of the 89 participants who reported a TEAE had gastrointestinal events. Most were mild to moderate. 37% of amycretin participants discontinued, though most discontinuations were for non-safety reasons (withdrawal of consent, protocol violations). This high dropout rate is a feature of early-phase dose-finding studies with aggressive escalation — it doesn’t necessarily predict Phase 3 retention.
Phase 2 — Type 2 Diabetes (Subcutaneous)
Presented: ADA 2026 Scientific Sessions (June 2026)
Participants: 262 adults with T2D inadequately controlled on metformin ± SGLT2i
Duration: 36 weeks
Doses tested: Six dose levels from 0.4 mg to 40 mg subcutaneous, once weekly
Results:
- Met primary endpoint (change in HbA1c) across all doses
- Highest dose: up to −1.7 percentage points HbA1c reduction from baseline of ~7.8%
- 89.1% of participants achieved HbA1c < 7%
- Up to 14.6% mean weight loss at 36 weeks
Safety: Consistent with earlier trials — predominantly GI adverse events, dose-dependent, mild to moderate.
Phase 2 — Type 2 Diabetes (Oral + Subcutaneous)
Published: November 2025
Participants: 448 adults with T2D on metformin ± SGLT2i
Duration: Up to 36 weeks
Results:
- Once-weekly subcutaneous amycretin: up to 14.5% weight loss (vs. 2.6% placebo)
- Once-daily oral amycretin: 7.6% placebo-adjusted weight loss at 36 weeks
- Significant HbA1c reductions with both formulations
This is important because it shows both delivery routes working in the same population. The oral version delivers less weight loss than the injection (expected, given lower bioavailability), but still clinically meaningful — especially for patients who would never self-inject.
Oral vs. Subcutaneous: What Patients Need to Know
This is the question that will define amycretin’s real-world impact.
The Injection (Subcutaneous)
- Dosing: Once weekly
- Bioavailability: ~100% (bypasses GI tract)
- Weight loss in trials: Up to 22% at 36 weeks
- Best for: Patients seeking maximum efficacy, comfortable with self-injection
The Pill (Oral)
- Dosing: Once daily (taken on an empty stomach, similar to Rybelsus)
- Bioavailability: Lower than SC (relies on SNAC absorption technology)
- Weight loss in trials: Up to 13.1% at 12 weeks (Phase 1 — short duration)
- Best for: Injection-averse patients, early treatment, maintenance, broader access
The oral formulation will almost certainly deliver less weight loss than the subcutaneous version at equivalent treatment durations. That’s a pharmacokinetic reality — oral peptide absorption is inherently less efficient. But if oral amycretin can deliver 15–20% weight loss over a full treatment course (which the early trajectory suggests is plausible), that would make it the most effective oral obesity medication ever developed.
And the access implications are enormous. Globally, injection-based therapies face barriers: needle phobia, cold chain requirements, training, cost, stigma. A pill removes most of those barriers overnight.
Is Amycretin Available Yet? The Honest Timeline
Let me be direct about this because I see a lot of confusion online.
Amycretin is not approved anywhere in the world. It is not available in the US, the EU, or any other market. It is an investigational drug in clinical trials.
Here’s the realistic timeline:
Phase 3 trials (AMAZE program):
- AMAZE 1 (obesity) started February 2026, enrolling ~1,150 participants
- Primary completion estimated: June 2029
- Phase 3 in T2D also being planned following the ADA 2026 data
US FDA approval (projected): Q4 2030 at the earliest (GlobalData estimate)
EU EMA approval (projected): Q1 2031 at the earliest
Bulgaria and Eastern Europe: Typically 6–12 months after EMA approval for market access, depending on national reimbursement negotiations. Realistically, we’re looking at 2031–2032 for availability in Bulgaria, assuming everything goes smoothly with Phase 3 results and regulatory submissions.
For context, the semaglutide journey from Phase 3 initiation to market availability in smaller European markets took roughly 4–5 years. Amycretin is following a similar timeline.
I know that’s not what many people want to hear. But this is the reality of drug development (talking as a former CRA) — Phase 3 trials take time, and they should take time, because that’s how we ensure safety and efficacy at scale.
The Competitive Landscape: Where Amycretin Fits
Let me put amycretin in context against the molecules we’ve been covering:
Retatrutide (Eli Lilly): Triple agonist (GLP-1/GIP/Glucagon). 28.3% weight loss in Phase 3 at 80 weeks. The raw weight-loss numbers are higher. But retatrutide is injection-only. No oral formulation in development.
CagriSema (Novo Nordisk): Combination of cagrilintide (amylin analog) + semaglutide (GLP-1 agonist). Two drugs mixed together, not a unimolecular agonist. 22.7% weight loss in Phase 3 at 68 weeks. Also injection-only. Missed non-inferiority vs. tirzepatide in REDEFINE 4 (23% vs. 25.5%). Novo is filing an NDA at the current dose and planning higher-dose trials.
Tirzepatide (Eli Lilly): Dual GLP-1/GIP agonist. Approved as Zepbound for obesity. 22.5% weight loss at 72 weeks. The current standard-bearer.
Oral semaglutide (Novo Nordisk): GLP-1 only. Rybelsus approved for T2D. Higher doses being studied for obesity.
Amycretin’s unique position: It’s the only molecule in late-stage development that offers both a competitive subcutaneous formulation AND a potentially game-changing oral formulation. If the oral version can deliver 15–20%+ weight loss in Phase 3, it becomes the most accessible effective obesity therapy on the planet.
That’s not just a commercial advantage. That’s a public health argument.
What Excites Me — And What I’m Watching?
Here’s my honest take.
The subcutaneous amycretin data is competitive. 22% weight loss at 36 weeks with no plateau is strong, but Phase 3 at longer durations will tell us where it truly lands. It’s unlikely to match retatrutide’s 28% at the top end, but it doesn’t need to. Different mechanism, different profile, different use case.
What actually excites me is the oral formulation.
13% weight loss in 12 weeks from a pill, with no plateau in sight. If that trajectory holds — and we need Phase 3 data to confirm — we could be looking at the first oral medication capable of delivering weight loss that competes with early injectable results.
That changes the game for primary care. For patients in countries where injection-based therapies are inaccessible or unaffordable. For people who simply won’t inject themselves. For long-term maintenance after initial injectable treatment.
The amylin mechanism also opens a distinct biological door. We’re not just layering more GLP-1 activity. We’re targeting a separate satiety circuit — the brainstem area postrema pathway — that GLP-1 agonists alone don’t fully engage. That’s a fundamentally different approach to appetite control, and the clinical implications may extend beyond weight loss into areas we’re only beginning to explore.
What I’m watching closely:
1. The AMAZE Phase 3 program. Will the oral formulation deliver 15%+ weight loss over a full treatment course? That’s the threshold that changes the conversation.
2. Long-term safety. The early data is reassuring — GI side effects consistent with the class, no unexpected signals. But we need years of data, not weeks.
3. The head-to-head story. How will amycretin SC compare to tirzepatide and semaglutide in longer trials? And can the oral formulation outperform oral semaglutide at higher doses?
4. Access and pricing. Even the best drug in the world doesn’t matter if patients can’t get it. The oral formulation’s real impact depends on pricing and reimbursement decisions that are years away.
The Bigger Picture
I keep coming back to the same thought.
We’re not just watching new drugs enter the obesity space. We’re watching the birth of metabolic medicine as a field.
Retatrutide showed us what’s possible with triple agonism — bariatric-level weight loss from an injection.
Amycretin is asking a different question: what if we could make effective metabolic therapy as simple as taking a daily pill?
Both questions matter. And both answers are coming from the clinical trial data we’re seeing right now.
The injection-only era of obesity pharmacotherapy may have an expiration date. And amycretin — if the Phase 3 data holds — might be what writes that date.
The CRA in me is fascinated by the dual agonist mechanism.
The pharmacist in me is thinking about real-world access and adherence.
And the evidence nerd in me is counting the days until AMAZE reads out.
Stay tuned. This story is just getting started.✌️
Key References
1. Dahl K, et al. Amycretin, a novel, unimolecular GLP-1 and amylin receptor agonist administered subcutaneously: results from a phase 1b/2a randomised controlled study. The Lancet. 2025;406(10499). [PubMed](https://pubmed.ncbi.nlm.nih.gov/40550231/)
2. Safety, tolerability, pharmacokinetics, and pharmacodynamics of the first-in-class GLP-1 and amylin receptor agonist, amycretin: a first-in-human, phase 1, double-blind, randomised, placebo-controlled trial. The Lancet. 2025. [ScienceDirect](https://www.sciencedirect.com/science/article/abs/pii/S0140673625011766)
3. Novo Nordisk Press Release: Subcutaneous and oral amycretin data published in The Lancet and presented at ADA 2025. June 2025. [GlobeNewsWire](https://www.globenewswire.com/news-release/2025/06/20/3102977/0/en/novo-nordisk-s-subcutaneous-and-oral-amycretin-data-published-in-the-lancet-and-presented-at-ada-2025.html)
4. Novo Nordisk Press Release: Zenagamtide shows significant A1C reductions with up to 14.6% weight loss in adults with type 2 diabetes — presented at ADA 2026. June 2026. [PR Newswire](https://www.prnewswire.com/news-releases/novo-nordisks-investigational-zenagamtide-shows-significant-a1c-reductions-with-up-to-14-6-weight-loss-in-adults-with-type-2-diabetespresented-at-ada-2026--302793124.html)
5. Novo Nordisk Press Release: Advances early-stage obesity medication, amycretin, to Phase 3 clinical development. 2025. [PR Newswire](https://www.prnewswire.com/news-releases/novo-nordisk-advances-early-stage-obesity-medication-amycretin-to-phase-3-clinical-development-based-on-early-phase-clinical-trial-results-in-people-with-obesity-or-excess-weight-published-in-the-lancet-302487500.html)
---
Disclaimer: Amycretin (zenagamtide) is an investigational compound. It has not been approved by the FDA, EMA, or any other regulatory agency. The data presented here comes from published clinical trials and company press releases. This article is for educational and informational purposes only and does not constitute medical advice.